Rising medical student, welcome to the start of your new life in health care!
An amazing adventure in helping people awaits you, but first you must pass that dreaded beast called medical school examinations.
With so much information waiting to be crushed into your exploding skull, figuring out which resources to use can be stressful. Do you go to lectures? Do you watch third-party videos? Do you form a study group or remain a hermit? And how can you possibly survive anatomy classes, especially if you didn’t do a medical science degree beforehand?
In this episode, Steve runs through some of the most popular medical school materials. Are you afraid of missing out on an important study resource because no one told you about it for your entire first year? Don’t worry. That’s an odd but valid fear.
Instead of suffering through trial and error, relax in this concise collection of the big options available to you. You don’t have to waste time searching for the best resources when many of them are presented to you here.
It’s ultimately up to you to choose the study methods that work best for you — but to do that, you first have to know what your options are!
Podcast
Resources mentioned
USMLE preparation and video lectures
First Aid
Pathoma
Doctors In Training
Flash cards
Anki
Brosencephalon
Anatomy
Essential Anatomy
Acland’s Video Atlas
Textbook atlases
Netter
Gray’s Anatomy For Students
Moore’s Clinically Oriented Anatomy
Podcasts and audio
Humerus Hacks
MedConversations
Goljan
OSCE videos
Geeky Medics
Other resources
Review notes
Toronto Notes
Video lectures
Dr Najeeb
Osmosis
Question banks
BMJ onExamination
Passmedicine
About the guest speaker
Steve Waring is a medical student from The University Of Sydney. He enjoys drinking coffee, eating bland vegetables and helping subsequent generations of medical students achieve their best.
Have you ever wondered what immunology is like? No?
Well, this is awkward.
Assuming you said yes to the above, this episode is for you.
As you go through your medical studies and even hospital training, you sure learn a lot of exciting facts. But who teaches you about real life? Where do you go if you want to learn what it’s like to be an immunologist? Or a gastroenterologist? Or an infectious diseases physician? Or if you want to find out about the hours and challenges and good and bad parts of a specialty?
While the textbooks don’t teach you what life in a specialty is really like, our superb speaker Dr Sean just might.
If you’re a junior doctor looking for a specialty to love or a medical student wanting to know more about your possible future, this is for you.
Podcast
About the guest speaker
Dr Sean Riminton is an immunologist and immunopathologist at Concord Hospital and Royal Prince Alfred Hospital. As well as his specialist clinical work, Dr Sean is an Associate Professor with The University Of Sydney.
Although Dr Sean is much too nice to do any boasting himself, he does boast a range of impressive achievements:
Fellow of the National Blood Authority of Australia
Advisor to the Plasma Fractionation Review and IVIg Criteria for Use Committee
Founding Chair of the Immune Deficiency Foundation of Australia
Designed and implemented the web-based ASCIA Register of Primary Immunodeficiency Diseases for Australia and New Zealand
Founding investigator on the Australia and New Zealand Antibody Deficiency Allele Study
It’s designed for junior doctors and medical students who are curious about different specialties and the real life side of medicine, not just the pathophysiology of it.
Hear these guests’ stories and learn from their advice, whether it’s immunology, surgery, gastroenterology or something else you’re interested in.
What is it? Well, it occurs when you pour too much salad dressing on your salad.
Why is that bad?
Because then your salad becomes worse than it initially was without the salad dressing.
And then you don’t win friends with your salad, because your salad tastes bad.
Calamity.
This is tragic, because salad dressing is designed to make salad better. Paradoxically, it’s made it worse.
Paradoxical undressing, on the other hand, is also an undesirable occurrence.
Is it when you take your clothes off and that ironically repulses people from wanting to sleep with you?
No, it’s not.
Rather, it’s a phenomenon that occurs in the final stages of hypothermia.
Hypothermia
Hypothermia is when body temperature becomes abnormally low. <35°C is a good guide.
This can be precipitated by events such as swimming in icy water or being exposed to harsh weather conditions.
Paradoxical undressing
You would expect a hypothermic person to feel extremely cold. You would expect, then, a desire to put more clothes on.
Paradoxically, in very severe hypothermia, this is not the case. As a stark precursor to death, victims in the final stages of hypothermia are seized by the urge to remove clothing.
A postulated mechanism is as follows:
Person is exposed to cold environment
Cutaneous and subcutaneous thermoreceptors detect cold, inducing peripheral vasoconstriction to conserve heat
Peripheral vasoconstriction occurs
This compensation is insufficient to maintain core body temperature
Person develops hypothermia
Vasoconstriction can no longer be maintained
Possibility: hypothalamic function is impaired, so it cannot control vasoconstriction normally
Possibility: vasoconstriction is an active, energy-consuming process from smooth muscle contraction, whereas vasodilation is passive from smooth muscle relaxation
Peripheral vasodilation occurs
Person feels hot and tries to take off clothes
More heat loss, so body temperature is lowered even further
Person dies
References
Wedin, B., Vanggaard, L., & Hirvonen, J. (1979). “Paradoxical undressing” in fatal hypothermia. Journal of Forensic Sciences, 24(3), 543-553. doi:10.1520/JFS10867J
When someone is dying in front of you from heart-related causes, there are 2 important things to know.
1. What you can do to help
Your options are simple:
Provide First Aid, if you have the qualifications and competency
Call an ambulance
Stand around gawking uselessly
2. What the condition is called
You must know the name of the affliction. This is so you can shout it out in an authoritative voice at unsuspecting people on the street, in order to sound smart.
In fact, you don’t have to restrict your know-it-all behaviour to the street; you can spontaneously yell “myocardial infarction” or “cardiac arrest” in any setting.
While in line at a coffee shop? Yes.
During a first date? Yes.
While deciding between brands of canned tomatoes at the supermarket? Yes.
It all works. However, remain aware that this might make you appear — quite unjustly — like an eccentric. It might also the reduce likelihood of a second date occurring.
So here’s the question.
What exactly is the difference between myocardial infarction and cardiac arrest? In both cases, the heart fails to some degree.
Myocardial infarction, also known as a heart attack, is from a lack of circulation.
For example, years of junk food lead to atherosclerosis. Fatty rubbish clogs the coronary vessels that supply the heart muscle. The blood supply to the heart becomes blocked.
And while hearts need love, they also need blood. No blood means no nutrients. No nutrients for a long period of time means the deprived heart muscle dies.
Cardiac arrest is from an electrical abnormality. As a result, the heart stops beating.
It’s like when you buy cheap batteries and your remote-controlled car stops working after 10 minutes. The electrical supply just isn’t right.
Myocardial infarction can lead to cardiac arrest, but this isn’t always the case.
References
American Heart Association. (2016, September 19). Heart Attack or Sudden Cardiac Arrest: How Are They Different? Retrieved from http://www.heart.org/
American Heart Association. (2013). Cardiac Arrest vs. Heart Attack. Retrieved from http://cpr.heart.org/
If you like controversy, there is a One Nation Party in Australia.
But wouldn’t life be more interesting with a Cannulation Party? Make well-calculated intravenous access sites, not war.
The minutes would run something like this.
OFFICIAL MINUTES OF THE CANNULATION PARTY OF AUSTRALIA
Foreword
Cannulation means putting a tube into a vein to deliver substances. The tube stays in the patient for a period of time.
Venepuncture, equivalent to phlebotomy, means accessing a vein to draw blood. It involves sticking a needle into a patient but not leaving any in-dwelling devices.
Agenda
Discussion of cannulation
Indications
Contraindications
Risks
Procedure
Discussion of venepuncture
Indications
Contraindications
Risks
Procedure
Item 1.1: Cannulation Indications
Rapid delivery of substances, such as fluid, antibiotics or contrast for imaging
Not to draw blood, although blood can be taken when the cannula is first applied
Why not oral? A patient might ask you this. Cannulation is for situations where quick bloodstream access is desirable, such as in sepsis, and oral delivery is unlikely to have the necessary effect. For example, gut metabolism might be an issue.
Cannulation is relevant when repeated access is needed. It certainly beats jabbing an unfortunate patient countless times.
Item 1.2: Cannulation Contraindications
Arteriovenous fistula
Mastectomy, lymph node issues
Trauma, burns, infection
For example, the standard procedure in cardiology is to use the patient’s left side, as the cardiologist approaches the patient from the right. This allows nursing staff convenient access to the patient’s left.
However, this can vary according to the patient’s situation; if the left arm has a contraindication, use the right one instead — unless that too has a contraindication.
Item 1.3: Cannulation Risks
Primary risk is infection
Secondary risk is haematoma
As with any procedure, other risks are imaginable. The main ones for cannulation are infection and, with a smaller chance, haematoma.
Importantly, sterile gloves are to be used during cannulation. As with any procedure, appropriate hand hygiene should be used throughout. For example, before and after touching a patient or before touching an aseptic field. If in doubt, it’s better to wash your hands too many times than not enough.
Even if there is no sign of infection, your hospital might have a maximum time for which a cannula can remain in a patient, such as 72 hours.
Item 1.4: Cannulation Procedure
Understand the indication
Why is cannulation requested for this patient?
What gauge cannula should be used?
Does the patient have any contraindications?
What site is most appropriate?
Gather equipment
Bung
Cannula
Chlorhexidine and alcohol swab
Dressing pack
Includes needle, syringe, gauze and stickers
Kidney dish
Saline bottle
Sterile gloves
Tourniquet
Introduce self
Explain procedure
Obtain consent
Apply tourniquet
10cm above the desired cannulation site
Find the target vein
Back of the hand is a common site
Standard practice is to work distal to proximal to avoid affecting the flow if an attempt fails
Look for veins that are visible and straight if possible
Remove tourniquet
Reduce patient discomfort as much as possible
Unpack dressing pack
Open saline bottle
Clean patient’s skin with chlorhexidine and alcohol swab
This lets the disinfectant dry while you reapply the tourniquet and put on gloves
Reapply tourniquet
Put on sterile gloves
Combine syringe and needle
Like when the Power Rangers combine to form their giant Transformer at the end of every episode — seriously, every episode
Use this to draw the saline from the bottle without touching the bottle
Although not a strictly sterile procedure like scrubbing before surgery, this no-touch technique preserves what is available of the aseptic field
Remove the needle
Dispose of it in the sharps bin
If no sharps bin is nearby, dispose of the needle in your kidney dish
Keep paper rubbish in a separate location so that you can simply tip the kidney dish contents into a sharps bin later on
This prevents you from digging around in the kidney dish for needles afterwards, which helps to avoid needlestick injuries
Put bung on syringe
Place gauze distal to cannulation site
Unpack cannula
Cannulate
Pierce the cannula needle into the patient’s skin
There is a degree of preference here, but a 15°-45° angle is standard enough
People will tell you to have the “bevel down”
That’s very confusing
No one even knows what a bevel is
The pointy end of the needle is shaped like a triangle
It just means to have the pointiest, longest part of the triangle at the bottom, closest to the patient’s skin
Once it’s in, advance the cannula part, not the needle
Retract the needle
Put the not-attached-to-the-syringe side of the bung on the not-in-the-patient’s-skin side of the cannula
Note that there are multiple techniques to choose from
Another school of thought is an angle in the 15°-30° range
Much closer to the 15° side is advised
After you see flashback, ensure the needle is as close to parallel to the vein as possible
Advance the needle a small way to ensure you are in the vein and not merely subcutaneous
Then advance the cannula part
Tip
What hurts the patient the most is the needle being moved through the skin, which produces an unpleasant sting
Although hesitation is natural at this point, piercing the skin incompletely or slowly only complicates the process
It is better to do the procedure confidently to avoid having to retry or prolonging the sting
Although you might wish to avoid inflicting pain on the patient, some pain is inevitable for this procedure and it is better to work through it quickly than to futilely try to avoid it
Remove tourniquet
Flush with saline
This checks that the connection is patent
A test of any abnormalities if you are in the wrong site, such as swelling
Put stickers on
Secure the cannula
Place the appropriate identification stickers on
Document in the patient notes
Item 2.1: Venepuncture Indications
Draw blood for analysis, such as coagulation studies, full blood count, EUC or other tests
Item 2.2: Venepuncture Contraindications
As with cannulation
See Item 1.2
Item 2.3: Venepuncture Risks
Primarily bruising or pain from failed attempts
Item 2.4: Venepuncture Procedure
Gather equipment
Alcohol swab
Butterfly needle
Cotton ball
Gloves
Cannulation and collection of blood for culture are considered sterile techniques
However, standard venepuncture does not require sterile gloves
As in gloves from a sterile pack
Not unclean gloves you picked up from the street
Don’t pick up gloves from the street
Tourniquet
Tube for blood collection
Vacutainer
Introduce
Consent
Apply tourniquet
Find vein of choice
Remove tourniquet
Unpack equipment
Merge butterfly needle and vacutainer
Alcohol swab
Wipe area clean
Reapply tourniquet
Put on gloves
Venepuncture
Pierce butterfly needle into vein until there is flashback
Like bevel, another fancy word that means nothing
It refers to blood visibly coming back through the tube
Hold butterfly needle still
Stop moving the butterfly needle if you see blood coming back, because that means you’re where you want to be
Advancing further could puncture through the other side of the vein
Despite the name, entirely puncturing a vein is not the aim of the procedure
Collect blood
Attach blood tubes to the other side of the vacutainer
Watch the blood pour in
Remove tourniquet
Remove butterfly needle
But remove the tourniquet first to avoid blood gushing in your face
Apply a cotton ball to the area
The patient can be asked to hold this
Sheath needle
Dispose of equipment appropriately
References
Australian National University. Intravenous cannulation. Medical Student Journal of Australia. Retrieved from http://msja.anu.edu.au/
According to one survey, top American fears in 2016 included:
corrupt civil servants
expensive medical bills
computers replacing human workers
clowns
people gossiping about you behind your back
But this research was wrong.
Do you know what’s more frightening than all of those things put together?
Without question, it’s Donald Trump dressed as a clown, waving a pricey medical invoice and shouting “YOU’RE FIRED!” behind your back, because you’re being replaced by a Surface Pro.
Yet there could be something worse: having your stomach rumble in the middle of a quiet lecture theatre.
To say that’s a little embarrassing might be a gross understatement for some.
Luckily, there’s a solution for that — eat more food.
Today, we’ll explore the art involved in selecting sustenance that is nourishing, tasty and able to be surreptitiously consumed in a small space.
For food to pass as lecture-worthy, there are 4 basic requirements that must be satisfied.
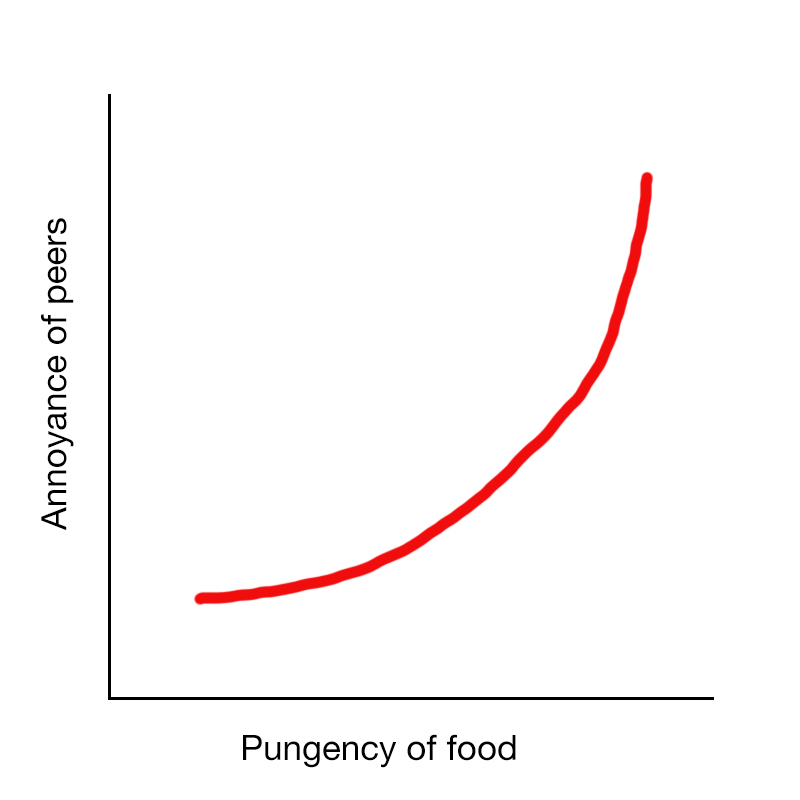
1. Smell
The relationship between aroma and public reception is well-established, with an excess of smell often sparking displeasure in others.
An increasing function best describes this phenomenon.
For this reason, hot food is generally to be avoided.
2. Noise
As humans have evolved to listen out for ringing phones and to enjoy bad pop music, their hearing can be quite sensitive. Thus, sound is an important consideration.
In the following graph, we see the impact of noisy food on audience disruption.
3. Practicability
Consider how much space is available around you and how space your meal preparation would require. Is there someone sitting next to you? Or do you have horrible body odour that drives everyone away, thus granting you a larger area? These factors can either limit or enable your culinary activities.
For example, filleting a fish might be tempting during a particularly mundane class, but the space requirements often prove too difficult to overcome.
Consider also the effort required. Pineapple would be refreshing in the middle of an intellectually rigorous lecture, but cutting it would involve a lot of mess and a lot of casualties.
4. Waste
Just like your crazy ex, some food comes with excess baggage. This is often in the form of a fruit skin or a plastic wrapper.
Unfortunately, there are risks in standing up to immediately dispose of rubbish. Most insidious is that of the lecturer suddenly stopping mid-sentence, looking pointedly at you, asking if you have a question and drawing the entire room’s attention to you.
The other option — to stockpile wrappers around you until the end of the class — is also unpleasant. As we all know, hoarding is a dangerous pastime with the potential for highly negative consequences.
Does your food of choice involve a haphazard amount of residue or wrapping? You might want to seek an alternative.
Here’s a reminder why.
With those principles in mind, let’s analyse some specific examples.
Banana: Silent and nutritious. Occasionally has a long-range smell. Be prepared to head straight to the bin after consumption. Otherwise, bring a plastic bag to store the leftover peel.
Breakfast bar: Delicious and convenient. Some types pose a crumbling risk.
Nuts: Cashews? Good. Almonds? Good. Peanuts? Good — but not for anyone nearby with an allergy. Pistachios? If there’s a risk of accidentally swiping the shells off your desk when you move your hand, and there always is, avoid.
Yoghurt: Bring a spoon to avoid ungraciously slurping from the container. As with bananas, rubbish is a concern.
Protein ball: Filling. As an added bonus, makes you look like a health aficionado.
Chocolate: A highly recommended lecture food. Good to share with others. Especially if you do have bad body odour and need to entice more people to sit near you.
Apple: Healthy but generally noisy. High crunch risk. A core remains after consumption.
Sausage roll: Warm, delicious and sure to create envy in all your neighbours. Some pastry varieties are particularly prone to breaking off into flakes.
Chips: Crunchy and involve rubbish. Similar to apples in this respect, except without any of the health benefits.
It’s the start of a new year, which means the start of another 365 days of procrastination.
The remedy for procrastination? An impending deadline, probably. Or behavioural economics, which is all about recognising and addressing inherent human biases; this lets you optimise the way you carry about your daily business.
But sometimes you need to use these biases to your advantage if you want to stop compulsively looking up pictures of cats in saucepans instead of studying…or if you’re prone to sitting on your fat ass all day.
It’s okay to use the word “ass”, right? Is this supposed to be family friendly?
3 things there:
Cats in saucepans are adorable.
A lot of people don’t like studying/dieting/exercising/[other productive activity]. They know they should do it but can’t bring themselves to.
Instead of trying to diminish your biases, you can harness them to work in your favour.
So let’s address and embrace these biases.
1. Sunk Costs
In an unprecedented moment of heated passion, or maybe when I referred to your fat ass above, you bought yourself a gym membership.
A gym membership is a sunk cost, meaning it’s already been paid for. While there’s not much you can do to recover it, you also don’t have to pay another cent; this fee is totally in the past.
Future decisions should take this into account by dismissing the sunk cost completely. So if you’re rational and you hate exercising, it makes sense for you to ignore the membership altogether.
You won’t receive your money back, so why put yourself through hours of pain for a lost investment? It’s better to let it go. So much for your New Year’s Resolution!
But if you allow yourself to be irrational, you can conjure up the fear of this money going to waste — even though it’s technically not — and use it to inspire positive action.
Whether it’s a gym membership, subscription-based study tool or expensive dieting program, the principle is the same. Pay for big commitments up-front and then stand by them to avoid feeling like you wasted your money.
Conclusion: Honour sunk costs.
2. Endowment
The endowment effect is a bias where you overvalue things you own. In essence, you’re scared of losses and hold on too tightly to what you already have.
Maybe you hate fur coats, especially ugly ones. But then your atherosclerotic life partner gives you the ugliest fur coat you could ever imagine. Oh, and you suddenly become Miley Cyrus.
Now you have a sentimental attachment to this fur coat, because it’s your ugly fur coat. It’s no one else’s. It’s yours.
Then disaster strikes. Someone breaks into your house and steals your ugly fur coat. Just that fur coat. Nothing else.
Now you feel the sting of losing the ugly fur coat, even though you’d been just as happy before you ever received it.
Why? Because you’re scared of experiencing losses and you place a high value on what you perceive you already own. Something that was yours was taken away and you don’t find that a fun experience.
Now here’s the effect it has on your New Year’s Resolutions. When your desire to change is expressed as a loss, it’s hard to follow through with it. Stop eating junk food? Stop reading useless things on the Internet? Wear less ugly fur coats? No, no, it’s all too hard to do.
Instead, rethink what your goal is. Maybe it’s to achieve better health. Maybe it’s to focus more on your study or work. Maybe it’s to improve your fashion sense. These are gains, not losses, and therefore feel more palatable.
Conclusion: Rephrase resolutions as things you will do instead of things you will stop doing.
3. Framing
Phrasing matters, doesn’t it? Actually, it matters a lot. How you express things deeply affects how you think about them.
The classic example is a village with 600 people. You have access to a medical program that saves 200 people. That sounds good, doesn’t it?
But you can look at it another way and say the program lets 400 people die. Although it’s the same thing, it suddenly sounds much worse.
Expression makes a difference, even if the things being expressed are exactly the same. In experiments, simply changing the wording affects people’s decisions.
So you know what? Use this to your advantage. To ensure your goals feel like successes, reframe the way you think about them.
Make your New Year’s Resolutions ridiculously easy. Make them achievable. Then reward yourself — focus on the positive and celebrate what you do achieve, not what you haven’t yet.
Because in the true spirit of procrastination, you can always do that later.
Conclusion: No matter how small the win, focus on what you do achieve rather than what you do not.
References
Lenton, P. (2016, December 30). Make your New Year’s resolutions kinder, and they’ll be more likely to stick. The Sydney Morning Herald. Retrieved from http://www.smh.com.au/
Thaler, R. (1980). Toward a positive theory of consumer choice. Journal of Economic Behavior and Organization, 1(1), 39-60. doi:10.1016/0167-2681(80)90051-7
Tversky, A., & Kahneman, D. (1981). The framing of decisions and the psychology of choice. Science, 211(4481), 453-458. doi:10.1126/science.7455683
You’re waiting at a bus stop in unfamiliar territory; on this exciting day, you’re going to a park you’ve never been to before. New park, new children to cruelly push off the swings. It sounds glorious.
According to the timetable, the bus you want to catch will arrive at 2:06pm. You prepare yourself for a small wait.
While sitting and picking your nose, you see another bus pull up. You ask the driver if the bus is heading to where you want to go, thinking it might be a shortcut.
“NO!” cries the bus driver emphatically. “In fact, the service you’re after doesn’t run on weekends! You have to go to the other bus stop down the street and wait there.”
This is not what the timetable says. But the bus driver is yelling at you and seems so sure. You ruminate as he trundles off.
Who do you listen to? That depends on who the credible authority is.
If bus stop information is regularly updated and results are correlated by searching a travel app or website, that could well be the credible authority. Recall that a bus driver can only vouch for his or her own route and, vitally, has no personal or reputational stake in whether you actually catch your bus or not. He or she might give you information believed to be true, but that doesn’t mean it’s correct.
However, suppose the timetable is not well-maintained. In fact, you notice the paper peeling as though it hasn’t been updated in many years. Furthermore, let’s say that drivers have knowledge across multiple routes. In that case, you know who the credible authority is.
Importantly, if you jump on bad information, it can take you far from your intended destination. You end up worse off than when you started. Even if the credible source says to wait a little, you’re better off doing that, because it will pay off in the long run.
Searching for trustworthy medical information is no different. Except there are no buses involved. And it’s totally different.
When you’re starting out, it can be tough to differentiate between credible and less credible sources. Unreliable sources are often littered with telling advertisements like “LOSE 4LBS IN 5 DAYS!!!!!!”, but this isn’t always the case.
Bad information is worse than no information. This is why looking in the right place matters.
How do you identify the right place? Look out for:
These are organisations that come from a trustworthy background, have a reputational interest to uphold or have been vetted for by someone who cares. With multiple other sources available, such as UpToDate, there’s little excuse for subscribing to bad information in this technological age.
It shouldn’t need to be said, but worryingly it still does: sites like howtogetbiggerboobsnaturallyfast.com are unlikely to be unbiased or trustworthy.
And it might be a personal bias, but staying wary of sites with keywords like “natural health advisor” or “homeopathic gluten free nutrition expert” has proved wise so far.